Artículo
SCN1A testing for epilepsy: application in clinical practice
Hirose, Shinichi; Scheffer, Ingrid E.; Marini, Carla; De Jonghe, Peter; Andermann, Eva; Goldman, Alica M.; Kauffman, Marcelo Andres ; Tan, Nigel C. K.; Lowenstein, Daniel H.; Sisodiya, Sanjay M.; Ottman, Ruth; Berkovic, Samuel F.; The Genetics Commission of the International League Against Epilepsy
; Tan, Nigel C. K.; Lowenstein, Daniel H.; Sisodiya, Sanjay M.; Ottman, Ruth; Berkovic, Samuel F.; The Genetics Commission of the International League Against Epilepsy
; Tan, Nigel C. K.; Lowenstein, Daniel H.; Sisodiya, Sanjay M.; Ottman, Ruth; Berkovic, Samuel F.; The Genetics Commission of the International League Against Epilepsy
Fecha de publicación:
05/2013
Editorial:
Wiley
Revista:
Epilepsia
ISSN:
0013-9580
e-ISSN:
1528-1167
Idioma:
Inglés
Tipo de recurso:
Artículo publicado
Clasificación temática:
Resumen
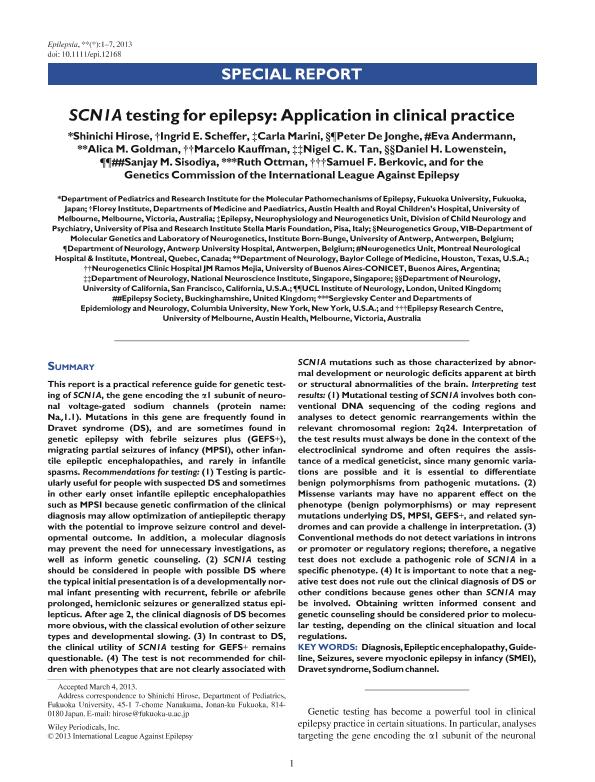
This report is a practical reference guide for genetic testing of SCN1A, the gene encoding the α1 subunit of neuronal voltage-gated sodium channels (protein name: Nav1.1). Mutations in this gene are frequently found in Dravet syndrome (DS), and are sometimes found in genetic epilepsy with febrile seizures plus (GEFS+), migrating partial seizures of infancy (MPSI), other infantile epileptic encephalopathies, and rarely in infantile spasms. Recommendations for testing: (1) Testing is particularly useful for people with suspected DS and sometimes in other early onset infantile epileptic encephalopathies such as MPSI because genetic confirmation of the clinical diagnosis may allow optimization of antiepileptic therapy with the potential to improve seizure control and developmental outcome. In addition, a molecular diagnosis may prevent the need for unnecessary investigations, as well as inform genetic counseling. (2) SCN1A testing should be considered in people with possible DS where the typical initial presentation is of a developmentally normal infant presenting with recurrent, febrile or afebrile prolonged, hemiclonic seizures or generalized status epilepticus. After age 2, the clinical diagnosis of DS becomes more obvious, with the classical evolution of other seizure types and developmental slowing. (3) In contrast to DS, the clinical utility of SCN1A testing for GEFS+ remains questionable. (4) The test is not recommended for children with phenotypes that are not clearly associated with SCN1A mutations such as those characterized by abnormal development or neurologic deficits apparent at birth or structural abnormalities of the brain. Interpreting test results: (1) Mutational testing of SCN1A involves both conventional DNA sequencing of the coding regions and analyses to detect genomic rearrangements within the relevant chromosomal region: 2q24. Interpretation of the test results must always be done in the context of the electroclinical syndrome and often requires the assistance of a medical geneticist, since many genomic variations are possible and it is essential to differentiate benign polymorphisms from pathogenic mutations. (2) Missense variants may have no apparent effect on the phenotype (benign polymorphisms) or may represent mutations underlying DS, MPSI, GEFS+, and related syndromes and can provide a challenge in interpretation. (3) Conventional methods do not detect variations in introns or promoter or regulatory regions; therefore, a negative test does not exclude a pathogenic role of SCN1A in a specific phenotype. (4) It is important to note that a negative test does not rule out the clinical diagnosis of DS or other conditions because genes other than SCN1A may be involved. Obtaining written informed consent and genetic counseling should be considered prior to molecular testing, depending on the clinical situation and local regulations.
Archivos asociados
Tamaño:
102.3Kb
Formato:
PDF
Licencia
 Excepto donde se diga explícitamente, este item se publica bajo la siguiente descripción:
Creative Commons Attribution-NonCommercial-ShareAlike 2.5 Unported (CC BY-NC-SA 2.5)
Excepto donde se diga explícitamente, este item se publica bajo la siguiente descripción:
Creative Commons Attribution-NonCommercial-ShareAlike 2.5 Unported (CC BY-NC-SA 2.5)
Identificadores
Colecciones
Articulos(IBCN)
Articulos de INST.DE BIOLO.CEL.Y NEURCS."PROF.E.DE ROBERTIS"
Articulos de INST.DE BIOLO.CEL.Y NEURCS."PROF.E.DE ROBERTIS"
Citación
Hirose, Shinichi; Scheffer, Ingrid E.; Marini, Carla; De Jonghe, Peter; Andermann, Eva; et al.; SCN1A testing for epilepsy: application in clinical practice; Wiley; Epilepsia; 54; 5; 5-2013; 946-952
Compartir

Altmétricas